= VIEWER DISCRETION IS ADVISED =
Have you ever asked yourself:
(1) Why wasn't I born a male with a penis?
(2) Why can't I not have period pains?
(3) Why can't I not give birth but have children?
(4) Why can't I play a more active role in sexual intercourse?
(5) Why can't I be a man?
(6) Why am I branded the
weaker sex?
(7) Why can't I have a penis to wank with?
(8) Why can't I be the US president?
(9) Why must I be the mother and not the father?
(10) Why am I such a lousy driver?
... and all the
"why nots" you could think of. Look no more, if you have had asked yourself the
why nots listed above, the solution is here. Read on. Again, viewer discretion is advised and if you're under the age of 18, please read the rest of the article without getting caught.
The following is a step-by-step guidethrough of a sex change op, female to male.
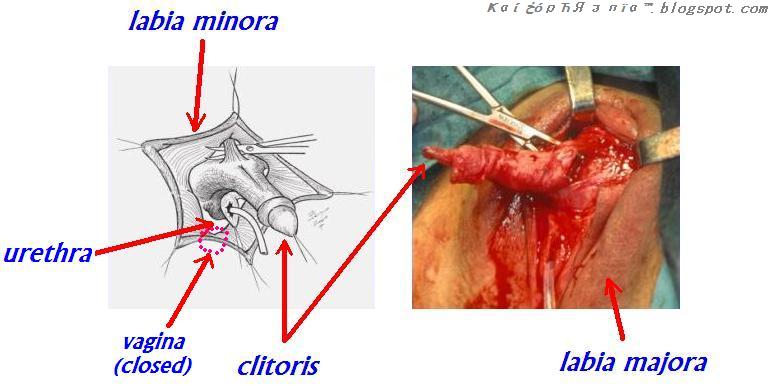
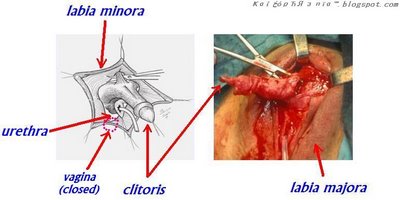
First, the surgeon would rip the
labia majora apart and make a deep incision to expose the root of your clitoris. A catheter (tube) would be inserted into your
urethra (your urine pipe) to drain any retained urine or blood.
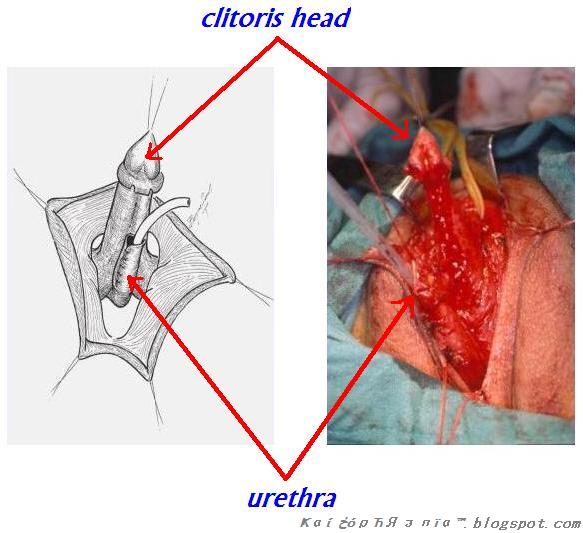
Further incisions would be made to further expose the whole length of your
clitoris and the
urethra.
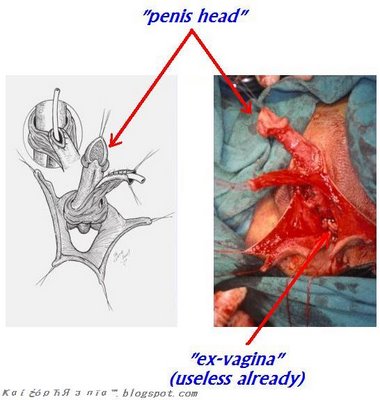
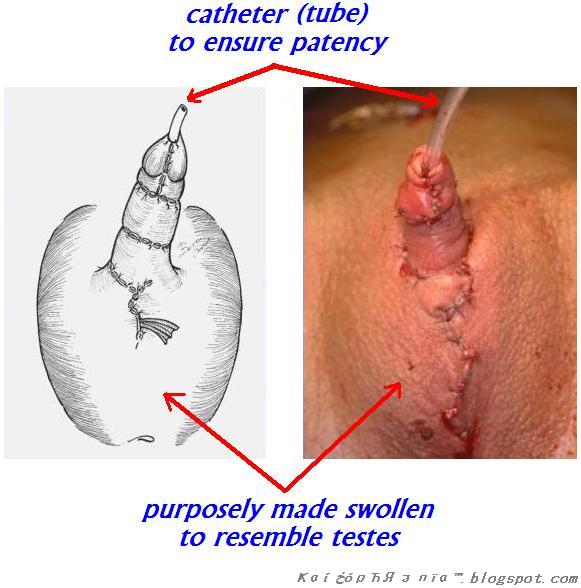
Next, tissue would be grafted along the length of your
clitoris and its glands to create the your new
penis. At this point it is essential to tell your surgeon before hand if you would like it to have a
prepuce or come fully circumcised. At this juncture, the opening of your
vagina would be sutured together, thus closing it.

The wounds are allowed to heal. Further reconstructions and refashioning of your newly acquired
penis may be needed to achieve maximal satisfaction, cosmetic wise. The last operation would be insertion of an inert material, such as silicone, to create the testicles. You may call it a pair of
silicone-balls or
silicone-nuts.
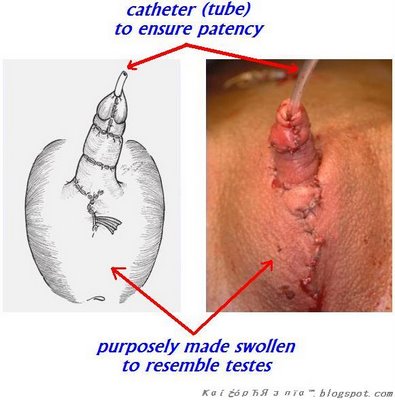
And voila! You have your new penis to play with. It may appear small initially (
baby-dick), but later on when revascularisation (growing of blood vessels) takes place, your new organ may grow in size, depending on the situation and mood.

 ҜαίخόρЋЯзпїα™
ҜαίخόρЋЯзпїα™
 This is NOT a blog!
This is NOT a blog! 
 Loading...
Loading...
 I'd finally survived a spontaneous vertex delivery from medical school on Feb 28, 2008! No meconium aspiration in the process, it was a clear pass. No resuscitation required. Am receiving my birth cert called MBBS in May, with my surname "Doctor" imprinted on it! Aahhh... the air is so refreshing...
I'd finally survived a spontaneous vertex delivery from medical school on Feb 28, 2008! No meconium aspiration in the process, it was a clear pass. No resuscitation required. Am receiving my birth cert called MBBS in May, with my surname "Doctor" imprinted on it! Aahhh... the air is so refreshing... With my mates
With my mates Kumpulan Kongsi Gelap Anti-Sosial
Kumpulan Kongsi Gelap Anti-Sosial With my group study members, "Kumpulan Gagak Hitam"
With my group study members, "Kumpulan Gagak Hitam"